
WRITTEN BY: Harrie Phillips
BAdVocEd (VocEd&Trng), RVN, DipVN (Surgical, ECC), DipBus, DipTDD, TAA.

Most veterinary clinics get their vet nurses to change their soda lime on a regular schedule or when the colour finally changes. But is this correct? Exhausted soda lime leads to unstable anaesthetics, and changing before it’s exhausted may mean you are throwing money away.
Soda lime absorbs carbon dioxide (CO2) through a complex chemical reaction, which also requires moisture to occur.
So ensure you store your soda lime as per the manufacturer’s instructions, and if your soda lime is sitting in the canister for any length of time, change it even if it hasn’t reached the 6 to 10 hours of use yet, as dehydrated soda lime cannot absorb CO2(1,6).
Soda lime is used with circle circuits (rebreathing circuits) and should be changed after every 6-10 hours of use*
*The manufacturer of the soda lime determines the specific recommendation.
Where does the CO2 come from?
Your anaesthetised patient exhales carbon dioxide.
Carbon dioxide is produced within the body through cellular function and transported to the lungs via the circulatory system for elimination. During respiration, in the pause between inspiration and expiration gaseous exchange occurs at the alveolar level within the lungs. Carbon dioxide is excreted and oxygen is absorbed into the blood. The carbon dioxide is then exhaled from the patient and will travel into the circuit and into your soda lime.
If your soda lime has exceeded its capacity to absorb carbon dioxide, and is still being used, these expired CO2 gases will recirculate to your patient through the anaesthetic circuit. This will likely result in hypercapnia, increased use of inhalation agent and oxygen, as your patient will require more of these to stay in an appropriate anaesthetic plane. Hypercapnia is a serious issue and can lead to hypotension, reduced organ perfusion, cerebral oedema, renal failure or even death1.
Does patient size matter?
As a general rule, the canister volume should be twice the patients’ tidal volume2,6, so smaller compact canisters will inherently have less capacity to absorb CO2. You may consider changing soda lime closer to 6 hours of use, if your clinic is using compact AAS KAB canisters or similar. For prolonged anaesthesia, large patients or when you have a smaller canister (or a combination of all), you may need to change your soda lime during the anaesthetic. This should be performed when a 50% colour change has occurred or if your ETCO2 baseline is increasing or if persistent hypercapnia is evident (ensure you have a spare canister ready!).
But what about the colour change?
Relying on the colour change alone to indicate exhaustion is not reliable3. Soda lime changes colour due to a different chemical reaction involving the pH (the manufacturers add this magical property in to help you determine when it might be exhausted). Soda lime often reverts back to its original colour after use (as the pH changes again) but this does not indicate that the soda lime has a restored capacity to absorb CO2 – it is still exhausted!
Dehydrated soda lime won’t change colour, as the chemical reaction cannot occur without moisture. This could lull you into a false sense of security, as no colour change will occur. You will notice that your patient is requiring increased amounts of inhalation agent to maintain anaesthesia and tachypnea with increased effort may be evident.
How else can I tell that the soda lime is exhausted?
Fresh soda lime is easily crumbled if you crush it between your fingers (whilst wearing gloves!). Exhausted soda lime (which can absorb no more CO2) will feel hard if handled.
Active soda lime heats up as the chemical reaction is occurring. If you feel the canister during an anaesthetic, it should be warm. If it is not warm, it is not working!
Can capnography help?
Capnography will allow you to measure CO2 concentration during patient expiration. This provides you with great feedback on the efficacy of your soda lime, as well as critical data on your patient’s status. If you are lucky enough to work in a clinic that uses capnography, you should be aiming to maintain ETCO2 between 35-40mmHg. Many capnographs will also show inspiratory CO2 (PiCO2) – you need to maintain this below 6mmHg4. Any higher and you should check your patient, check the circuit for kinks, look at the amount of dead space present and then assess your soda lime for exhaustion, as higher levels of inspired CO2 can indicate that your soda lime is exhausted.
Exhausted soda lime capnogram
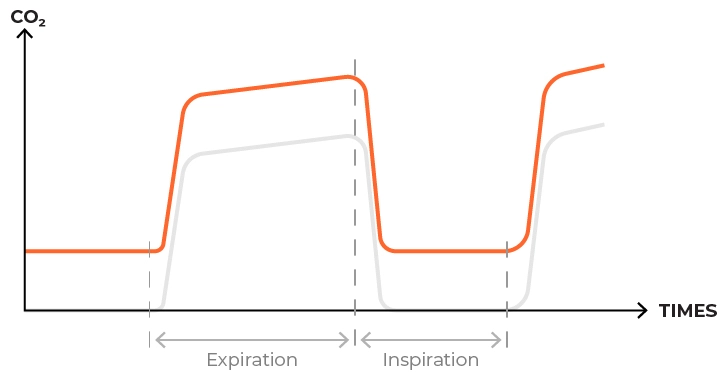
When your soda lime is exhausted, your Capnogram will look like the image above – whereby the baseline increases from 0 to higher, the higher the baseline sits at the more exhausted your soda lime is. The shape of the capnogram would otherwise look normal7.
So the question now is: How do you measure usage?
When you have demonstrated 6-10 hours of active use, the soda lime needs to be changed. If you do not reach 6-10 hours of use within a week you may consider changing your soda lime anyway, as it will be slowly drying out. Remember, moisture is required for the chemical reaction in the soda lime to occur, ensuring that carbon dioxide is absorbed 6. Check the soda lime manufacturer’s instructions for storage criteria and length of time the bottle can be ‘open’ on the shelf.
Here is a FREE Soda Lime Usage Chart that you can download, print, laminate and attach to your anaesthetic machine to fill in. Registered ACVN Training Clinic? Ask us to send you a free plastic one!
How to Use: When you are using a rebreathing circuit that utilizes soda lime, simply place a cross or your initials in a triangle after every 15mins of use.
Changing Soda Lime
When changing soda lime ensure you are wearing gloves and mask, and perform the change in a well ventilated, low traffic area. The soda lime should be firmly (but not too tightly) packed within the canister5. Ensure all air pockets between the granules are removed. Loosely packed soda lime is not as efficient at CO2 absorption as the gas will flow through these air pockets, taking the path of least resistance2. Pack too tightly and you increase circuit resistance and impact the patient’s ability to ventilate efficiently. Take care not to overfill your canister, most canister manufacturers recommended leaving a small gap at the top, the size of this will depend on the size of the canister.
Refer to your canister and soda lime instructions at all times.
Hint: If you can feel some hot spots and some cool spots (during use) then the soda lime is not packed properly.
References
1 Anaesthesia Learners Guide, Veterinary Nurse Solutions; Phillips H, 2012
2 BSAVA Manual of small animal anaesthesia and analgesia, 1st edition; Seymour & Gleed, 1999
3 Hall, Clarke & Trim, 2001, p. 57
4 ACTA Anaesthesiology Taiwan. 2004 Dec;42(4):199-202. The valid time of soda lime could be safely prolonged according to the inspired pressure of carbon dioxide. Chen YH1, Chen CL, Chung YT, Yeh LT, Lu KT, Lin CY.
5 5-Minute Anesthesia Consult; Nina Singh-Radcliff, 2012
6 Anaesthesia for Veterinary Nurses, edited by Liz Welsh
7 http://www.veterinary-equipment.net/1731/detect-soda-lime-exhaustion/
want to learn more?

ANAESTHESIA & SURGICAL ANALGESIA
SHORT COURSE
This course introduces students to the foundations of anaesthesia – how to set up and test the equipment, what circuits to pick and when, calculations, and other factors that can influence how stable our anaesthetics are. You’ll also learn how the drugs we use affect the body, patient warming techniques and important and why premedication is necessary. We also explore analgesia specific for surgical patients.
Check it out